

Key insights
- CMS is using the LEAD ACO model to encourage more providers into accountable care relationships tied to quality, cost, and patient outcomes.
- Participant providers are directly tied to alignment, quality reporting, and payments, while preferred providers can support care coordination with less direct exposure.
- LEAD includes risk-sharing options, benchmark adjustments, capitation payments, and quality withholds, so participation decisions should be modeled carefully.
- Whether you are already in a value-based model or exploring one, assess your risk appetite, provider relationships, data capabilities, and value proposition before moving forward.
Explore LEAD ACO opportunities and evaluate your options.
For more than a decade, Medicare has worked to shift providers from volume-based payments toward paying for the value of care received. Accountable Care Organizations, or ACOs, sit at the center of that shift.
An ACO in the words of the Centers for Medicare & Medicaid Services (CMS) is a “group of health care providers that has chosen to come together to take accountability for the quality and Medicare total cost of care for their aligned beneficiaries.”
The newest ACO entry is the Long-Term Enhanced ACO Design, or LEAD.
How LEAD ACO fits into Medicare accountable care
ACOs come in many forms across Medicare, Medicaid, and the commercial market, but they share a common goal: holding providers accountable for both the quality and the cost of care delivered to a defined patient population.
CMS has a goal of having all Medicare enrollees in an accountable care relationship for quality and cost of care by 2030. Two ACO programs dominate Medicare today:
- The Medicare Shared Savings Program (MSSP) was written into statute under the Affordable Care Act and is the oldest and largest ACO, covering roughly 12.6 million beneficiaries.
- The REACH ACO model — Realizing Equity, Access and Community Health — has 1.7 million beneficiaries. It sunsets December 31, 2026, and is replaced by the LEAD ACO launching January 1, 2027.
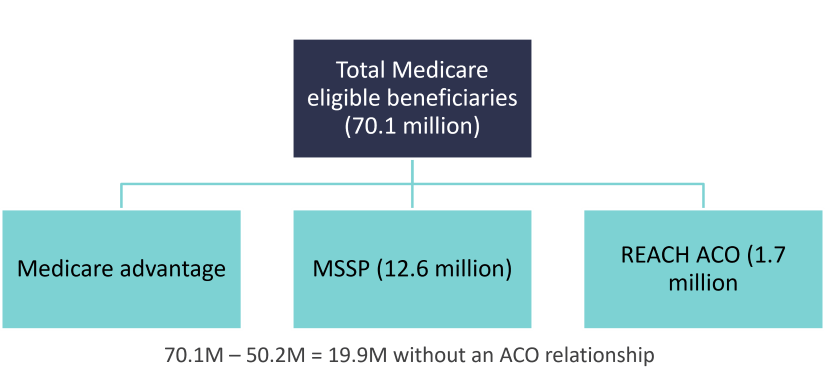
In total, ACOs and Medicare Advantage represent 50.2 million beneficiaries — Medicare Advantage with 35.9 million and ACOs with 14.3 million. This leaves roughly 20 million remaining only without any connection to accountable care and in traditional fee-for-service.
LEAD is the next iteration of ACOs and CMS is looking to engage more into accountable care models by addressing problems exposed under earlier models.
Who can participate in the LEAD ACO model
LEAD ACOs are structured as “whole TIN” approaches: Participation is managed at the tax identification number (TIN) level, meaning Medicare-enrolled providers or suppliers billing under a participating TIN take part as a “participant provider.”
This could include physician group practices, networks of individual practitioners, hospitals employing physicians, Federally Qualified Health Centers, Rural Health Clinics, and Critical Access Hospitals.
These participant providers are used in beneficiary alignment to the ACO, quality reporting and capitation payments. In other words, they are directly part of the ACO. Patients are connected to an ACO either through claims-based alignment — based on where they receive the plurality of their primary care — or by voluntarily aligning themselves to a Participant TIN.
LEAD ACOs may also include “preferred providers.” Preferred providers don’t count toward alignment or quality requirements, for example, so are indirectly involved in the ACO’s outcomes.
Preferred providers help the ACO facilitate care management across settings or services, thereby improving quality outcomes and managing spend for the ACO’s patient population. They can access waiver flexibilities and have the option of participating in capitation payment agreements but don’t have to. Preferred providers participate at the TIN-NPI (national provider identifier) level.
Preferred providers tend to be specialists or post-acute care providers.
How LEAD ACO payments and risk-sharing work
LEAD’s financial methodology is where much of its complexity lives. Benchmarks start from an ACO’s historical baseline expenditures calculated over three years (2024 through 2026). Benchmarks are adjusted (regional efficiency, risk adjustments), trended, and have certain withholds (quality and a built-in discount).
ACOs choose between two risk-sharing options — professional risk at 50% or global risk at 100%. This is the shared savings or shared risk the ACO will take on for their patient populations.
ACOs also choose their capitation payment option — either primary care or total cost of care. Capitation payments — per member per month payment the ACO receives — are designed to provide up-front funding and move away from volume-based billing.
With capitation payments, participant providers and suppliers in the ACO and those preferred providers who elect to use capitation payments don’t receive claims-based reimbursements for the specified services covered by their capitation payments.
LEAD ACOs have other options as well, such as advanced payments, non-primary care capitation, and CMS-administered risk arrangements (CARA).
LEAD quality measures and performance requirements
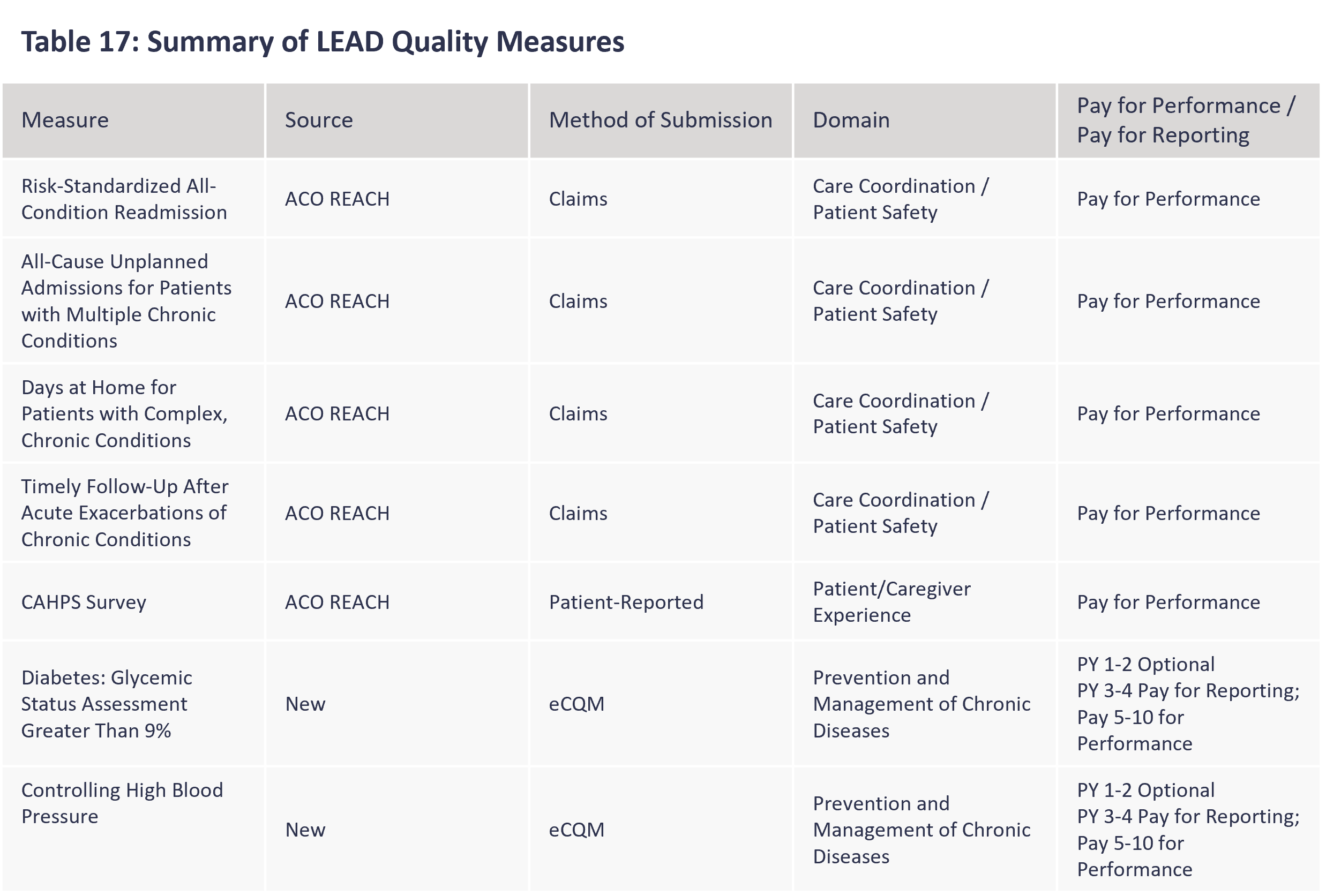
Quality isn’t an afterthought in any value model. LEAD requires a quality withhold of 3% of the benchmark which ACOs can earn back through meeting quality performance measures and other requirements. The measure set should be familiar to REACH ACOs since it uses five current measures. Two new measures — diabetes and high blood pressure — are optional in a model’s first two years but become mandatory after that.
CMS also wraps the model in supporting infrastructure — a Tech Enabler Initiative, a Rapid Cycle Innovation Program, and learning systems designed to spread effective practices quickly.
Why LEAD matters for value-based care
LEAD represents Medicare’s bet that a more flexible, risk-calibrated, prevention-focused ACO can encourage more involvement and better care.
For those weighing participation, such as hospitals and physician practices, the details matter, as there are real opportunities for meaningful upside savings but the same is true for financial exposure. The model also provides new opportunities for other providers, such as post-acute care and specialists to test out the value-based waters with less exposure as preferred providers.
ACO Involvement
| Potential Pros | Potential Cons |
|---|---|
|
|
How CLA can help with LEAD ACO planning
The value-based landscape continues to evolve. LEAD is the next step in testing new ACO policies, offering new opportunities for sophisticated value-based organizations or to those looking to get into the game.
If you’re thinking about any value-based model as a participant or preferred provider, consider these starting questions:
- What is your experience (or comfort level) with risk-based contracts (one or two-sided)?
- Are you in a model currently? Does that preclude you from joining another model?
- What are the potential upsides for model involvement (e.g. increased revenue, data/analytics, technology tools)?
- For preferred providers looking to join an ACO, what’s your value proposition?
As you evaluate LEAD or any ACO model, CLA can help assess financial exposure, model scenarios, review provider arrangements, and identify reporting or data gaps.
Contact us
Explore LEAD ACO opportunities and evaluate your options. Complete the form below to connect with CLA.